How long has humanity been plagued by cancer? The answer might surprise you. It looks like our ancestors faced the same challenges as we do in the 21st century.
Some of the earliest proof of cancer is found among ancient mummies from Egypt. Archaeological evidence suggests that people of the past suffered from the same types of tumors as people do nowadays.
However, ancient Egyptians had no clear understanding what cancer is and hence no effective therapies existed. The cause and cure for the dreaded disease have always remained a mystery. (Ref.)
Fortunately, in the last century the progress in understanding oncological diseases has been tremendous. When anesthesia became available, surgeons rapidly developed operations that removed the entire tumor along with cancerous lymph nodes. (Ref.)
During World War II, compounds blocking critical chemical reactions for DNA replication emerged. Further development of such cytotoxic agents led to the advent of chemotherapy. Unfortunately, these drugs targeted normal cells as well as cancer cells, therefore, safer yet effective alternatives were still needed. (Ref.)
Before long, more sophisticated treatments such as immunotherapy and targeted therapy became available in oncology. The better understanding of cancer biology resulted in new age medicines. These medications could boost the immune system’s response to target malignant cells and hinder cancer growth, division as well as metastasis. (Ref.1), (Ref.2)
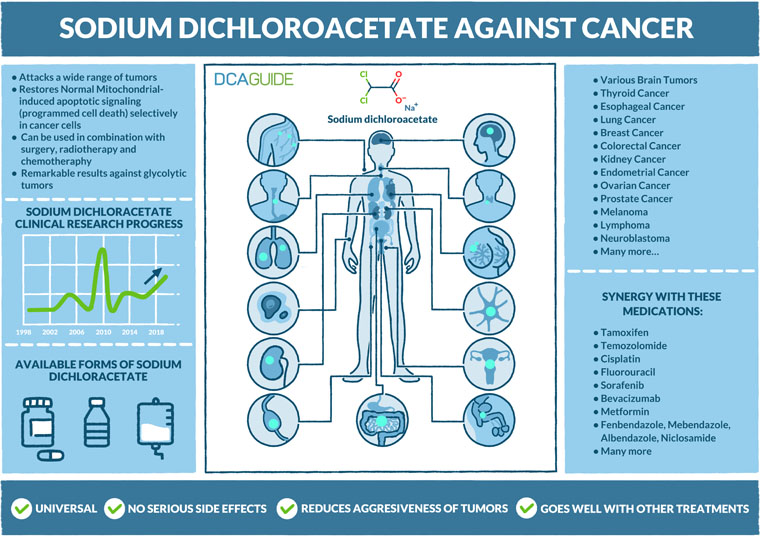
Interestingly, the whole exploration process led to unexpected discoveries. Significant metabolic shifts were acknowledged to be a characteristic of many cancer types. Coupled with the emerging wave of drug repurposing these findings opened the door for metabolic cancer treatment and soon Sodium dichloroacetate became the most prominent example of this strategy. (Ref.)
Cancer metabolism
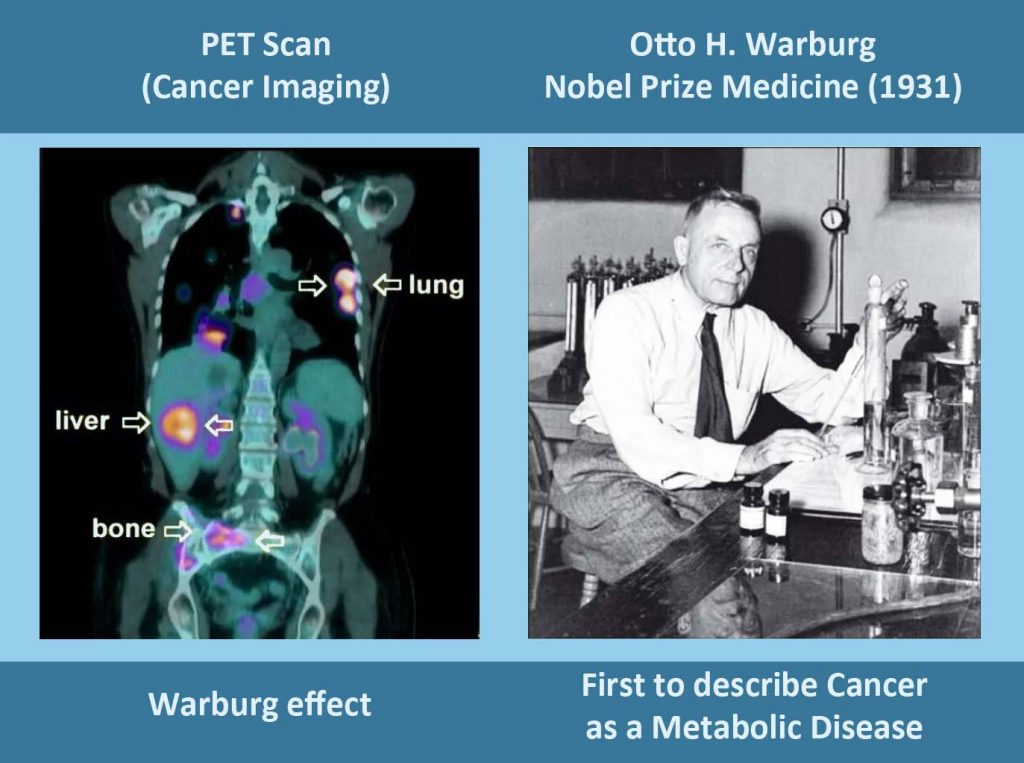
In 1923, a German biochemist, medical doctor and Nobel Prize laureate, Otto Heinrich Warburg, made a ground-breaking discovery vital in understanding the energy metabolism of cancer cells. This identified phenomenon is now recognized as the hallmark of cancer and is called the Warburg effect.
Otto Warburg observed the cells of a rat tumor and noticed that their growth is powered by extreme amounts of glucose (sugar) without the increased use of oxygen. This made no sense since using oxygen for producing energy from nutrients is a significantly more efficient way. Over a hundred years ago such findings raised more questions than answers.
Now it’s known that the enormous glucose hunger and reduced intake of oxygen grant cancer cells a unique set of evolutionary advantages. (Ref.)
One of the ways how cancer cells benefit from the Warburg effect is by shifting to rapid biomass production. The increased glucose uptake provides the cancerous tissue more building components for making new genetic material and protein, ultimately leading to increased cancer proliferation and growth. (Ref.)
In addition, it is well known that normal mammal cells are constantly supplied with oxygen, otherwise they would die quickly. However, malignant cells act in a totally different way. As the tumors grow rapidly, they often outgrow their oxygen supply. Needing no oxygen to fuel its growth and thrive, the cancer does not suffocate.
Soon the tumor cells switches its metabolism to aerobic glycolysis. It begins producing and excreting excessive amounts of lactic acid outside the cells, eventually leading to increased acidity of the tumor microenvironment. (Ref.)
Acidic tumor microenvironment promotes further invasion and metastasis by breaking down the extracellular matrix between our cells. Once the acidity level is elevated, it also helps cancer development in avoiding our immune system, the natural defense mechanism against malignancies. This is one of the reasons why the effect of immunotherapy can often start diminishing when treating advanced cancer. (Ref.)
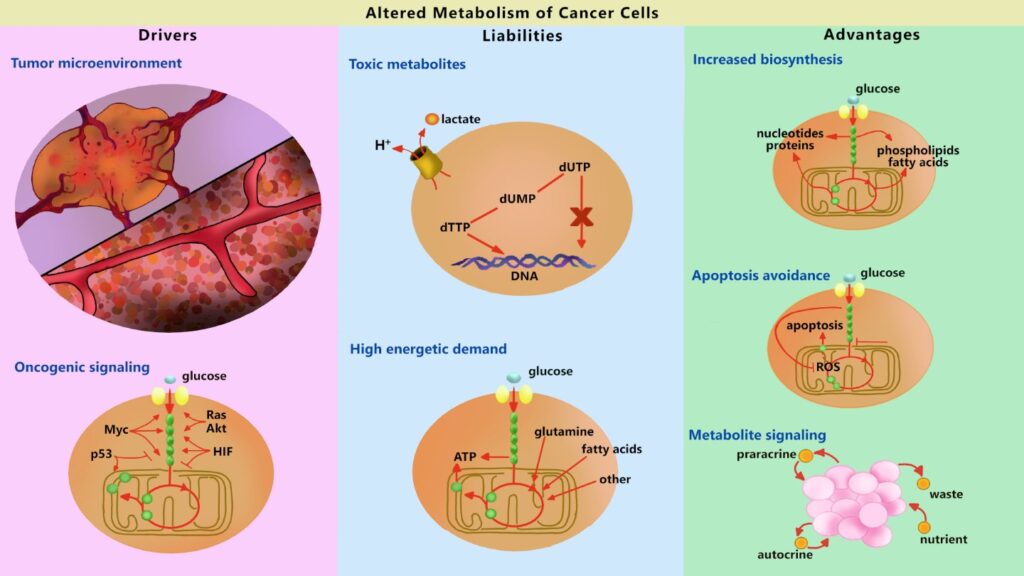
At the same time, the tumor cells utilizes less oxygen, the mitochondria inside the cells start generating less reactive oxygen species that serve an important role in preventing as well as removing cancerous cells. The cancer begins avoiding a mechanism known as apoptosis. (Ref.1) (Ref.2)
Apoptosis is a normal process that occurs in our organism as a convenient way to eliminate cells that should no longer be a part of the body. It’s a form of natural programmed cell death that prevents tumors from developing and expanding in the first place. As a consequence of avoiding apoptosis, the cancer cells become immortal. (Ref.1), (Ref.2)
These are the main metabolic advantages that enable the tumors to thrive. Notably, the evolution of tumor cells is a rather complex process, which makes it a difficult disease to treat. However, this is just one side of the coin. On the other hand, the Warburg effect can be exploited against the cancer itself.
In diagnostics, humanity used this cancer metabolism phenomenon for diagnostics. The positron emission tomography (PET) scan reveals the tissues and organs that have abnormal metabolic activity.
Since the cancer cells have the Warburg effect active, they absorb radioactive glucose a couple of hundred times faster than the surrounding normal tissue. As a result, the tumors light up in the images and can be conveniently traced in the whole body. (Ref.)
In treatment, the Warburg effect could be the “Achilles’ heel” of cancer that was ignored for almost a century, since virtually all of the past cancer therapeutics focused on a gene-centered approach. The compound Sodium dichloroacetate acts in a completely different manner and instead corrects the abnormal metabolism of the cancer cell.
How DCA treats cancer?
It disrupts the chemical reactions that tumors use for their rapid growth, starving cancerous cells of nutrients. Moreover, it restores the “bad” metabolism in cancer cells. DCA is an activator of damaged mitochondria.
As a consequence of stimulating the mitochondria, DCA increases the production of reactive oxygen species in the cell. These changes induce further cellular mechanisms that lead to apoptosis, which in other words is selective tumor cell death. This results in decreased proliferation of cancer cells, decreased tumor size, symptom alleviation and increased host survival. (Ref.)
DCA treatment transforms the most aggressive cancer cells to less aggressive ones. Since the Warburg effect is only present in malignant cells, healthy cells remain unaffected by Sodium dichloroacetate.
What positive improvements to expect?
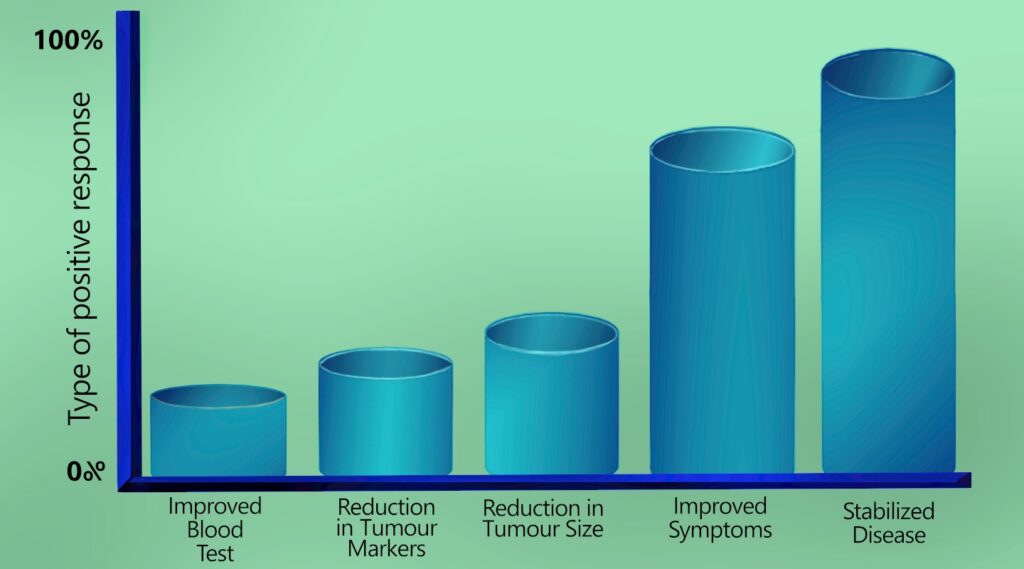
DCA is great for stabilizing the tumors, which means that they cease to grow and expand. This also leads to improved well-being and reduced tumor markers of the patient.
People can expect to regain their appetite, strength and weight. DCA also treats the chronic pain that is often present as a complication of cancer development.
In addition, Sodium dichloroacetate is also an option for someone with brain tumors since it crosses the blood-brain barrier.
Dr. A. Khan explains the benefits of DCA in his excellent lecture.
How to use DCA for cancer?
DCA should be used as a single agent or in combination with other regimens until there is no evidence of disease (NED) in the cancer patients.
Even when the cancer is gone, it’s advisable to continue using DCA for cancer at least 5 years in lower doses and have prophylactic screening once every 3-6 months. If the cancer is away even after 5 years, DCA treatment can be used in low doses occasionally as a prophylaxis to ensure that the tumors don’t come back.
We will finish this page as soon as possible. In the meantime, please use our DCA dosage and usage (Quick guide) or DCA dosage and usage (Long guide).
Cancer cells and DCA-resistance. How to overcome this problem?
The Sodium dichloroacetate molecule enters the cancer cell through the SMCT1 (SLC5A8) transporters.
Unfortunately, as the tumor tissue becomes more malignant and develops more mutations, the expression of the SMCT1 transporter goes down. Subsequently, DCA has a harder time entering the cells to produce its maximum anticancer effect. (Ref.)
If one has experienced a dramatic improvement at the beginning of DCA cancer treatment and after some time the effect has been diminished, it could mean that the tumor has developed some drug resistance to DCA. Nevertheless, there could be a practical solution to this issue. (Ref.1), (Ref.2)
Diclofenac 25 or 50 mg tablets orally 1-2 times per day can lead to the re-expression of DCA transporters. It also serves as an anti-inflammatory drug and a pain killer, which could help oncological patients manage physical pain.
The problem with Diclofenac is that it also suppresses the gastric mucosal barrier, which might lead to the stomach acid causing heart burn or small erosions. In more severe cases, it can cause peptic ulcers and bleeding if used for prolonged periods of time.
The solution to this problem is the additional use of proton-pump inhibitors such as Omeprazole (Prisolec), Pantoprozole (Protonix), Lasonprazole (Prevacid) or Esomeprozole (Nexium) 20 mg once daily, 30 minutes before breakfast. These medications reduce stomach acid secretion and thus prevent the most common Diclofenac-associated side effects. (Ref.)
Furthermore, there is evidence to suggest that Omeprazole enhances the effect of DCA. (Ref.)
The protocol to overcoming DCA-resistance in tumors:
- Diclofenac 25 or 50 mg one tablet once or twice daily, at least 30 minutes before breakfast and/or dinner (total 25-100 mg per day). Five days a week, two days break. Resume.
- Omeprazole (ideally), or Pantoprozole, or Lasonprazole, or Esomeprozole 40 mg once per day, at least 30 minutes before breakfast, daily, without breaks.
Examples: A) 160 lb person with no cancer-associated pain and diminished response to DCA therapy should take Diclofenac 25 mg twice daily with Omeprazole 40 mg in the morning. B) 220 lb person with moderate cancer-associated pain and diminished response to DCA therapy should take Diclofenac 50 mg twice daily with Omeprazole 40 mg in the morning.
*Diclofenac should not be used if one has severely impaired kidney function, liver disease, history of erosions or ulcers in the upper gastrointestinal tract, bleeding due to clotting disorders or asthma.
*Omeprazole or other proton-pump inhibitors should be avoided if the individual has osteoporosis, a broken bone or systemic lupus.
Ibuprofen, ketoprofen, fenoprofen, naproxen, indometacin, resveratrol and quercetin are not recommended with the DCA cancer protocol, since they tend to worsen the transportation of the DCA molecule into the cancer cells through the deactivation of SMCT1 transporters. (Ref.1), (Ref.2)
The evidence suggests that taking vitamin E supplements could actually undermine the cancer-fighting effects of DCA. (Ref.)
This is because procaine, which is not recommended for use in restoring SMCT1, has poor bioavailability and can only theoretically work in cell laboratory cultures. (Ref.1), (Ref.2)





















My wife just finished a 30 day supply taken with DMSO (1000 mg) and FB (2000 mg). MBC ++ her2-. Scans right before Christmas…. no new growths, some existing getting smaller. On other meds as well. No side effects from DCA.
We do take breaks. 4 days on and 3 off. There are other supplements you need to take with it. Please read up about it.
Does DCA work on Bone Metastasis from the kidney. I’ve been taking it for about 2 weeks now.
Has anybody using DCA experienced chest pains?
I’ve been taking DCA regularly since my diagnosis. The research shows that it doesn’t work on all varieties of my cancer. I had a period of 3 months without chemo while I was doing surgeries and my cancer grew and spread despite the DCA. Now the chemo that has been working very well this past year has stopped working and the cancer is growing again despite my use of DCA. Is it safe to increase the dosage and if yes, how much?
Some have increased to 50mg/k along with increasing their Alpha Lipoic Acid, Carnitine and Benfotiame while I have heard from some that actually claimed to add that Fendbendazole along with their protocol and achieved more positive results. While not sure about it as i havent tried it myself but you could look up online who has and perhaps ask direct how they did while using it.
As to the higher doses of DCA for aggressive cancers, it has been utilized but you have to closely monitor for toxic reactions to the dead cells slophing off as they tax the kidneys so detox is also important to clear out system, which by increasing fluids considerably can help lower the cincentration of dead cells for your body to eliminate.
Avoiding sugars and junk carbs helps to slow growth as they feed tumors.
High protein diet is considered to work well with most cancer treatments including when using DCA as well.
After taking DCA for 2 months my CT scan showed that my tumors were stable and there has been no growth. Is this a good sign after two months? Is 2 months to soon for them to be gone? I have a rare sarcoma, stage 4, with mets to lungs.
I got this and Essaic tea for my Aunt who had cancer in her stomach area (which the doctors could not determine exactly), and she couldn’t undertake any more radiotherapy, so they gave her chemotherapy. The doctors weren’t very hopeful, given that they couldn’t perform surgery because of other complications, and they were also worried that it may spread to her spine. I purchased DCA for her in May after watching some YouTube videos, and then in September she came back cancer-free. I’m not a physician, so I can’t confirm that it actually worked, but the result was there. Though I’d like to believe that my purchase was effective, like I said, I’m not a medical professional. I would still recommend it to anyone who needs it.
I cannot express how well dca worked for me; it has been effective without any side effects. By the looks of it, it is much safer than chemotherapy and any other treatments prescribed by an oncologist. Many thanks!!
Just wanted to give some hope to anyone fighting this battle or helping someone fight the battle. Just had my 3 month scan. I was diagnosed a year ago with stage 3 small cell lung cancer. I started DCA protocol right before brain radiation. My first scan after this I was NED! To be honest I was scared thinking the world would think I’m crazy. But my heart said I had nothing to lose. I’ve also never ever mentioned a word to my doctors about taking any vitamins or this protocol.
I thank God every day for another day! As a cancer survivor with little over one year in remission now and several years of testing and checkups to go. I can assure you I know the meaning of being thankful down to the level of every breath taken.
Great news! Praise God! My recent biopsy’s have shown that my pancreatic tumor is dead! They only found necrotic debris and non-viable tissue.
DCA cancer protocol worked for me. Metastatic 2 x 2 cm lung tumor and invaded lymph nodes totally gone on PET/CT scan after 17 weeks
Dear DCA Guide, I’ve been recently diagnosed with gastric cancer in a fairly advanced stage. So far I have received no chemo. Where I live administrative barriers are high. Which is why I have purchased DCA capsules (500 mg) as well as Fenbendazole capsules 222 mg. I intend to begin taking both simultaneously as soon as my orders arrive. On the ‘DCA for cancer’ page on your website (section ‘Cancer cells and DCA-resistance. How to overcome this problem?’) you recommend taking Diclofenac and Omeprazole if the tumor develops resistance. Hence is my question: Does it make sense to include the latter two into the protocol from the very start of the course of treatment? Or would it be more reasonable to wait and see if there is indeed tumor resistance in my case? Needless to say, that I would like to avoid loss of precious time. Thank you for your reply in advance. Miroslav
I was diagnosed 4 years ago today with triple negative breast cancer! Have been NED since June 2022! All Glory goes to God!
Can you take DCA when you’re on chemotherapy? My friend has stage 2 breast cancer and just started chemo (she had the removal surgery 4 weeks ago) with three more months to go.
6 month CT Scan results today. My oncologist said, “completely normal”! God has kept me All Clear for 3 years 5 months! Prayers answered! Never quit never give up no matter what!
Can DCA be used in conjunction with mistletoe (viscum album) cancer therapy?
My husband was diagnosed 8/21 with non Hodgkin’s lymphoma after being cancer free for 5 years. He started taking the DCA protocol the next month and the lump on his neck disappeared within weeks.
I’m curious if you have any details regarding the synergistic use of Fenbendazole or Mebendazole to reduce tumors.
I started taking DCA very early November. A recent scan showed some existing tumors doubling in size, some stable-ish and some fast growth in other tumors. I wish you all the very very best in your healing journeys!
So many people and animals suffer from cancer each year and are told there is nothing more that can be done. To hear that there is hope out there using a combination of drugs not used by conventional Drs or vets is something we should be aware of and more research should be carried out especially as it could save lives and cost less than conventional treatments. It is something many of us may need in the future for ourselves or our pets. Thank you for this information and I hope it can save other lives in the future.
My father also did this protocol and he lived 43 months post diagnosis
I had Stage 2 Breast Cancer and coming up on 5 years remission. Praying the same for all of you!
Does fenbendazole kill cancer stem cells? or just the mature cancer cells?
As far as I know fenbendazole doesn’t have the ability to kill cancer stem cells. But on the other hand it has been used to treat certain types of cancer, and mostly effective against mature cancer cells.
Is there anyone here who has pancreatic cancer stage 4 , who decided to not do chemotherapy and only treating it with DCA? Would you mind sharing and tell me your protocol and how long have you been doing it.
Hi. I’m 64 years old, diagnosed w. Pancreatic cancer -(Advanced, local adenocarcinoma stage 3; 2.6cm tumor) a few months ago. Initially I was opposed to chemo & had hopes of getting into a clinical trial involving Immunotherapy. I didn’t find one I’m a candidate for & decided I’d do chemo. There have been holdups & delays getting a Pet scan & I’m on the fence about chemo after hearing about Neuropathy & other side effects. Been doing DCA protocol. Recent scans show that tumor has not grown. I feel pretty good- very little pain, ok appetite, weight loss has stopped, no jaundice, great energy.